At IWK Health, we are working to improve health outcomes during the transition from pediatric to adult care.
Transition from pediatric to adult health care is defined as the purposeful, planned movement of adolescents with chronic medical conditions from child-centred to adult-oriented health care (Blum, 2002) that is supported by individualized planning in the paediatric and community settings, a coordinated transfer of care and secure attachment to adult services (CAPHC, 2016)
The Transition of Care Committee has outlined the importance of a consistent structure for transition to ensure that youth have a similar experience across the Children's Health Program, noting that each patient & family and each care team will have unique needs and strengths that will necessitate flexibility within the framework.
The Transition Framework was developed by the Transition of Care Committee with support from the Transition Community of Practice.
The Transition Framework is informed by:
- National Guidelines on Transition from Children’s Healthcare Canada
- Research evidence on transition, including our local research and international consensus studies
- Guiding Principles, Values and Health Indicators for Transition developed by the Transition of Care Committee
- Ongoing feedback from youth, families, healthcare providers and community partners from across the Maritimes
The Transition Framework also reflects the recent Canadian Paediatric Society’s Call to Action on Transition
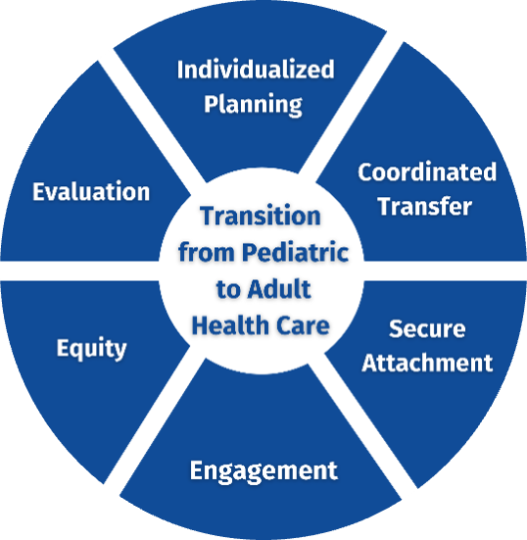
To improve the transition from paediatric to adult health care, we focus on six components of care:
Engagement
· Incorporate feedback from youth and caregivers into our practice
· Outline to youth and caregivers how their feedback has influenced our transition practice
Equity
· Consider how health equity plays a role in transition outcomes
· Consider how complexity of care plays a role in transition outcomes
Individualized Planning
· Assess youth’s health care skills
o Readiness Checklists, including youth’s health and advocacy goals, are completed early and consistently, and placed on the health record
o This assessment may be about the family’s knowledge to navigate adult care on behalf of their youth
· Have a system to track transition progress
o Clinic letters include a ‘Transition’ heading outlining youth’s progress on health goals and transition planning completed during the visit
Coordinated Transfer
· Discuss transfer of care with youth and family one year prior to transfer
o Care team supports the continued engagement of primary care in early adolescence and throughout the transition process
· Ensure youth and caregivers know how to access care during transfer
o Information about how and when to access preventative, urgent, and emergency care during the transfer period is consistently reviewed
Secure Attachment
· Support trust building with adult and primary care services
o Providing positive, informed guidance on adult care helps to manage expectations and engage youth and caregivers in care
· Provide additional supports to youth who face barriers to secure attachment
o Social and structural drivers of health and complexity of care effect transition outcomes. Addressing health equity is key to improving outcomes
Evaluation
· Set & track goals for transition processes and/or outcomes
· Collect data to demonstrate improvement in transition practice & health outcomes during the transition to adult care
If you would like more information about the Transition Framework, please reach out to our Transition Coordinator.